I’ve had plenty of vertigo in the past, but I wasn’t dizzy at all when I fell. I just bent over to pick up a heavy pot, and tipped right over. Sometimes when hiking on hills I’ll lose my balance, and I’ve fallen a couple of times. I’m in my 70’s, is this normal?
Read more: Help! I fell after bending overFalling never seems normal, but it becomes more common as we age. All parts of our balance systems begin to decline, and gradually it becomes easier to fall. That means you have to take active steps to prevent hurting yourself.
One of the most common balance problems comes from a gradual loss of sensation in the feet and lower legs. The nerves that supply the feet have to stretch from the spine, where the main part of the neuron resides, all the way to the feet. Any problem along this extension can result in a loss of feeling, and this is frequent in older people. Get a cold metal object like a heavy spoon and run it along your fingers; you can easily feel the cold. Now run the same spoon over the bottom and sides of your foot. If you find numb places, or don’t feel the cold as strongly, you are losing sensation in the feet. This can also be tested by placing a vibrator or vibrating tuning fork on your feet and comparing that to your hands. A loss of vibratory sense correlates with a general loss of sensation.
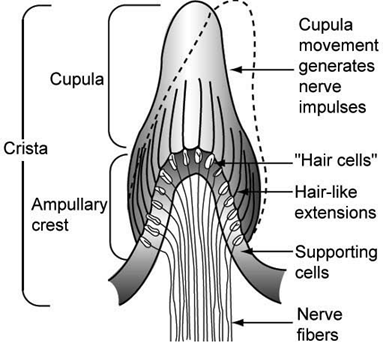
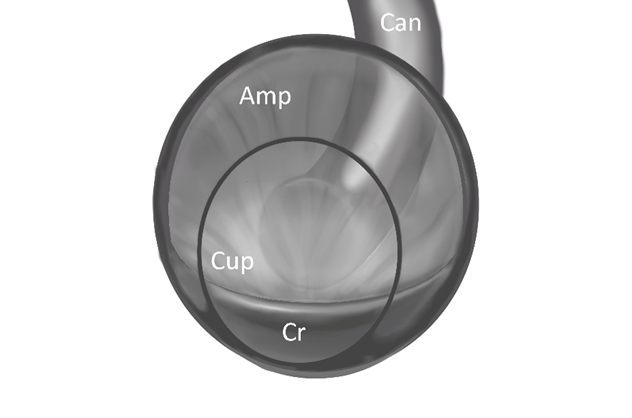
Why would losing sensation in the feet make you more likely to fall? The three components of the balance system are the inner ears (which sense movement of your head in space), your eyes (which can see whether you are upright, moving or tilted), and the feeling in your legs and feet. Even if your inner ears are functioning well, you still need some input from the other two systems.
When you bend over, you can no longer use vision for balance as well. Normally we use the horizon, or vertical objects near us, to measure whether we are stable. If we are still, the horizon stays horizontal and vertical things like trees or walls look upright. If we bend over to look at the ground, we lose that vertical and horizon orientation. It’s much harder for the balance system to detect a bit of tilt in that position.
That forces us to rely upon the feeling in our legs and feet for balance. If I can feel the ground, and tell whether my ankles are bending, then I know I am stable. It doesn’t take much loss of feeling to make this less effective. A little numbness makes you more likely to fall when you bend or focus on the ground instead of the world around you. You also become more likely to fall when in the dark.
Fortunately there is something you can do when this happens. In most people, sensation remains very good in the hands even if they lose some in the feet. By touching something stable like a wall or post, the tendency to tip over when bending forward will be stopped. Using trekking poles in the hands while walking has a similar effect. You will basically be bypassing your numb feet and allowing your hands to feel the ground through the pole, which will restore your balance.